CRNA Scope of Practice Explained
The Nested Umbrella Visualization

I recently came across a court case where a physician anesthesiologist allegedly refused to perform an emergency C-section, claiming it would be illegal to do so while medically directing a CRNA in another room. Tragically, this decision led to a preventable adverse outcome with lifelong ramifications for the family and resulted in a multi-million-dollar settlement.
That case really got me thinking and inspired this post. I'm often surprised by how little is understood about the Certified Registered Nurse Anesthetist (CRNA) scope of practice, even among hospital administrators, physician anesthesiologists, and, at times, fellow CRNAs.
This isn’t intended to be an exhaustive legal review (no one wants to read that on a Friday), but rather a broad and general summary for those who are curious—or for those who may find themselves, like the anesthesiologist above, potentially vulnerable in a high-stakes situation.
What Determines CRNA Scope of Practice?
Think of CRNA scope of practice as concentric circles or nested umbrellas, each layer representing increasing specificity:
Federal regulations – the broadest circle or umbrella
State laws and regulations – the middle circle or umbrella
Facility-level policies and privileges – the smaller circle or umbrella
While each layer can make CRNA practice more restrictive, none can expand it beyond what’s permitted at the higher level. For example, a hospital bylaw cannot allow a CRNA to perform something prohibited by state law or federal requirements.
Let’s walk through each level:
Federal Level: CMS Regulations and Billing
The federal government doesn’t define CRNA scope of practice in the clinical sense—but it does shape practice through Medicare billing rules and Conditions of Participation (CoPs) for hospitals.
Medicare Part A – Conditions of Participation (CoPs)
Hospitals must meet certain standards to participate in Medicare. For anesthesia services, the CoPs require that:
CRNAs administer anesthesia “under the supervision of the operating practitioner or of an anesthesiologist who is immediately available if needed,” unless the state has opted out of this requirement.
As of today, 25 states have opted out of this federal supervision rule. In the others, CRNAs may be “supervised” by a physician anesthesiologist or by the surgeon or proceduralist (e.g., gastroenterologist). However, CMS has never clearly defined what "supervision" means beyond being immediately available.
Medicare Part B – Billing Modifiers
CRNA practice is also influenced by professional fee billing models, which define how services are reimbursed. Every anesthesia claim must include a billing modifier that reflects the anesthesia care model:
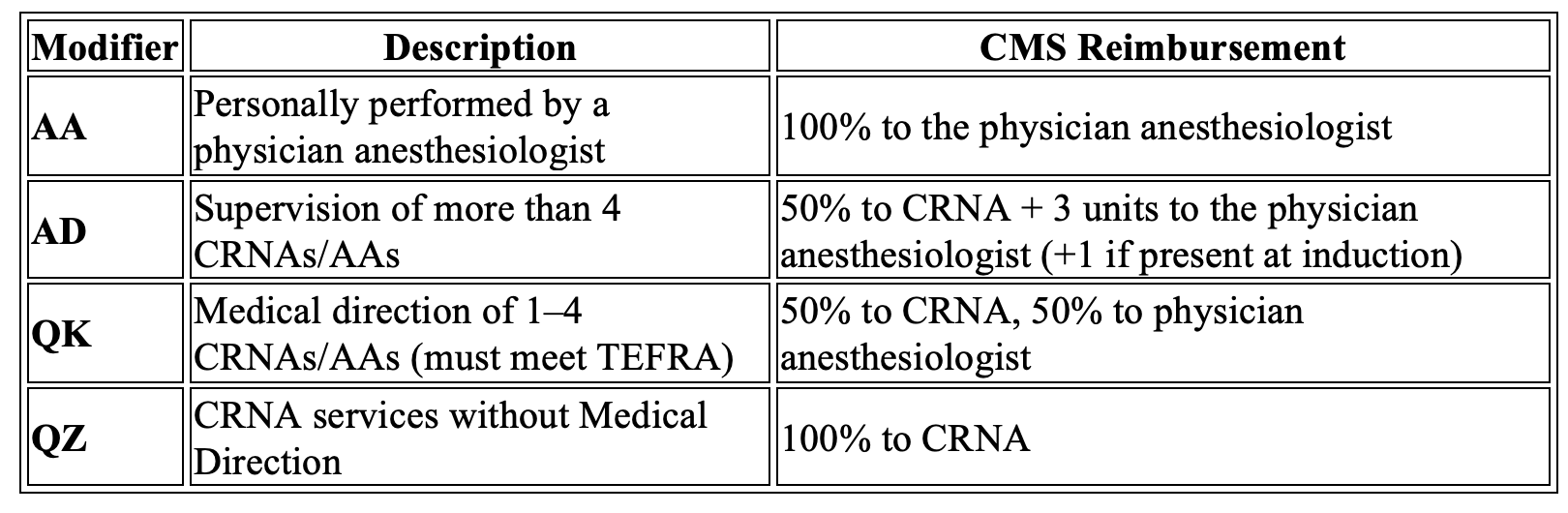
The 7 TEFRA Steps (Required for billing QK):
Pre-anesthesia exam and evaluation
Prescribe the anesthesia plan
Personally participate in key portions (induction/emergence)
Ensure other tasks are performed by qualified personnel
Monitor the patient at regular intervals
Remain physically present and available
Provide post-anesthesia care
Failure to comply with these steps while billing as “medically directing” can result in denied claims, fines, or even allegations of fraud.
State Level: Nurse Practice Act and BON Rules
Each state governs CRNA practice through:
The Nurse Practice Act (NPA): Statutory law that defines the scope of nursing practice.
Board of Nursing (BON) Rules & Regulations: Administrative law that provides detailed interpretation of the NPA. BONs may also issue opinions or declaratory statements, which can carry the weight of law in specific cases.
Additional state regulations may apply to other specific areas such as:
Office-based anesthesia
Chronic pain practices
Dental or plastic surgery settings
These often fall under state medical, dental, or pharmacy boards and can vary widely.
Facility Level: Bylaws, Policies, and Privileges
At the facility level, CRNAs must adhere to:
Medical staff bylaws
Delineation of Privileges (DOP)
Institutional policies and protocols
Even when a state permits a specific CRNA practice, individual hospital policies, bylaws, or delineation of privileges can impose additional restrictions. It is essential that Hospitals and CRNAs are aware of, and operate within, the specific privileges granted to them at each facility. While hospitals are legally allowed to be more restrictive than state law, this should be carefully weighed. In the event of an adverse outcome, providing care outside of hospital policy, even if within state scope, may increase the risk of liability for both the facility and the CRNA.
Why It Matters
Violating any of these layers of scope can have serious consequences:
Civil fines and penalties
Medicare audits or repayment demands
Disciplinary action by the Board of Nursing
Loss of licensure or hospital privileges
Negative patient outcomes—and in the worst cases, legal liability
In the case that inspired this post, care was allegedly withheld, not due to a lack of skill or availability, but for fear of violating billing compliance of Medical Direction where the CRNA case could have easily been billed under another modifier such as QZ and the physician anesthesiologist could have rendered the emergency care that was needed. The result was devastating. And no court will accept “I didn’t know” as a sound defense.
Final Thought:
Determining CRNA scope of practice is complex but visualizing it as a series of concentric circles or nested umbrellas can help clarify how the rules operate—starting with federal CMS billing regulations, then state Nurse Practice Acts, and finally, hospital bylaws and privilege documents.
It’s critical that all stakeholders—CRNAs, hospital administrators, physicians, and policymakers—understand these layers. We must continue to raise awareness, educate one another, and advocate for clear, consistent, and fair practice laws that allow CRNAs to work to the full extent of their education and training. Doing so is essential to meet the growing public need for safe, high-quality anesthesia care across the country.
Knowing your scope isn’t just smart—it’s essential.
Thx!
Well done.